Scientific progress rarely develops in a linear, steady fashion. Though volumes of data are always accumulating, the theories they ‘fit in’ take time to adjust in light of new or anomalous findings. The concept of paradigm shifts, developed by the philosopher Karl Popper, is a reminder that groundbreaking ways of thinking are always around the corner when it comes to scientific knowledge.
The emergence of neuroplasticity these past few decades is a strong example of this. In a departure from its earliest assumptions, contemporary neuroscience has accepted that the brain is not fixed as it reaches adulthood. Our central nervous system is highly malleable to experience and can reorganize and adapt to changing circumstances. This has had profound impact on medicine
In his book The Brain That Changes Itself, Dr. Norman Doidge tells the story of neuroplasticity with an eye for this historical lens. He takes us through rehab centers, laboratories, and clinics around the globe to explore how the dynamic ability for the brain to change itself is being used therapeutically. His mission is clear: to shed light on the groundbreaking feats of those he calls ‘neuroplasticians’, who are empowering their patients to grow in ways they might not have thought possible.
Brains on the mind
The brain’s complexity has yet to be fully deciphered by neuroscience. Unlike the heart, whose mechanics are known to the slightest movement, the brain’s neural pathways are still largely uncharted. Unlike the liver, whose function is reducible to specific biochemicals, the brain’s activity can only be broadly associated with certain neurotransmitters. But most significantly, no other organ can be said to contribute to your most intimate and immediate experience: your feeling of being you.
The ancient Egyptians hadn’t yet recognized the role of the brain in constructing human subjectivity. In fact, they attributed something like a soul to the heart instead: during ritual preparation of a body for mummification, it was safeguarded, while the brain was scooped out through the nostrils. Post-Aristotelian Greek medicine finally connected the brain to the ‘rational soul’, and in the centuries following, the idea that major executive decisions were the products of our brain grew. Guided by his live dissection of monkeys, Galen concluded that the brain controls muscles throughout the body by means of thread-like nerves. Nearly 2,000 years later, his theory has endured the test of time.

But as we know, the brain is responsible for much more than bodily sense movement: it‘s also the seat of the mind. We first started to understand this connection by studying how selective damage to animal brains would influence their behavior. These are referred to as ablation experiments, and the underlying concept is simple enough. If we have a complicated machine that gives us certain outputs, we can try to understand how it works by breaking some parts and seeing what stops working. The French physiologist Jean Pierre Flourens pioneered ablation experiments in the 19th century, providing important empirical grounds for the idea that subjective experience is constructed by the brain.
It took the work of Paul Broca, another Frenchman, to provide a further important clue to the brain’s activity: specific parts control specific functions. This idea, called localizationism, was initially rejected by many neurophysiologists in favor for an alternate theory called equipotentiality. Flourens himself espoused this latter view, maintaining that sensation, perception, and volition were a single faculty which “occupy concurrently the same seat”. By conducting autopsies of neurological patients, however, Broca was able to associate a specific part of the brain with the motor production of speech. Damage to this region, which now bears his name, causes a speech disorder called expressive aphasia in which patients are unable to articulate their thoughts but can understand language perfectly. This experimental finding elevated localizationism as the major paradigm of neurophysiology: for better or worse, as we’ll soon see.
“No, Donny, these men are (neurological) nihilists”
With localizationalism at its helm, neuroscience ventured into a detailed investigation of the brain and its sub-regions. This is best exemplified by the extensive work of Korbinian Brodmann, who examined and categorized the regions of the cortex — the outermost layer of the brain — according to the shape of their neurons. What resulted was an almost obsessively-detailed map of the brain which Brodmann believed could later be associated with specific functions.

Indeed, Brodmann’s areas do correspond to specific functions, as localizationism would predict. Areas 1, 2, 3 correspond roughly to the somatosensory cortex, which is responsible for processing incoming sensory stimuli. Areas 4 and 6 correspond to the motor cortex, which projects its signals out through the spinal chord and allows us to move our muscles. These findings, and hundreds more, showcase an organizational structure of the brain which relegates distinct functions to separate parts. Broca’s thesis has been vindicated.
However, localizationism also brings us a stubborn implicit assumption. When a certain region is damaged, the function associated with should be lost forever. After all, there is a 1:1 relation between function and location. This assumption has guided medical sciences in the pre-neuroplasticity era.
Modern-day research into neuroplasticity is starting to suggest otherwise. This is where Doidge formally introduces us to neuroplasticity. The paradigm of localizationism, he argues, has cultivated a mindset that he calls ‘neurological nihilism’: the idea that some neurological disorders are beyond hope. This is closely related to the concept that certain abilities are ‘hardwired’ into the brain, a theory which necessarily maintains that if the relevant wires are broken, the ability can never be recovered.
In direct opposition to neurological nihilism, Doidge tells us the stories of multiple patients who triumphed over their conditions with the help of neuroplasticity. Many of these are cases which would have been considered ‘beyond help’ by a more rigid interpretation of the brain’s functioning.
As a doctor himself, Doidge is driven by his own experience working with neurological and psychiatric patients. But he is also driven by a deep conviction that our current era — the ‘neurological revolution’ — will hold the key to new treatment plans which utilize developments in neuroplasticity. These treatments will put the dynamic nature of the brain to use, and by so doing, empower patients to recognize that their conditions can be alleviated by their prolonged efforts.
Here, I’ll present two specific cases from Doidge’s book which exemplify his project and the fundamental paradigm shift he attests to. The first is from the realm of medical neuroscience; the second is from the world of psychoanalysis.
The first of these showcases a stunning pathway to recovery which utilized the ideas of plasticity, and by so doing, resisted all the odds.
The power of cross-sensory plasticity
Homer, the near-mythical compiler of The Iliad and The Odyssey, is said to have been blind. The allure of this theory consists of the idea that, having his sense of sight compromised, the bard was uniquely predisposed to memorize and recite those thousands of lines detailing the heroism of antiquity.
We’ve all heard of the idea that when one sense disappears, another becomes stronger: a blind man who develops exceptional hearing, for example. This is more than just a psychological phenomenon: it reflects specific kind of neural rewiring called cross-modal plasticity. The occipital lobe, for instance — that region in the very back of the brain which processes visual information — has been shown to process auditory signals in blind patients.
This is an incredible testament to neuroplasticity. The brain can physically alter its neuronal pathways, reaching new targets and strengthening connections, to make use of a neglected and stimulus-deprived region.
Doidge introduces us to the clinical research of Dr. Paul Bach-y-Rita, who has been taking advantage of cross-modal plasticity in order to treat blind patients. In the 1970s, he invented a tactile vision device which feeds the contrast information of a given image into a configuration of vibrators on a metal plate. Contrast intensity is then converted into the intensity of vibration on the mechanical device. In this way, the patient can ‘see’ the image by feeling it on his/her back and eventually learn to detect and differentiate between objects.
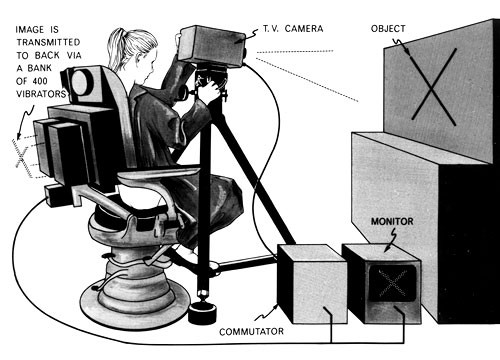
This device is a powerful example of sensory substitution. The sense of sight is being substituted by the sense of touch, such that many of the functional capacities that a seeing person could accomplish (discriminating against objects, detecting the distance of an object, and so on) is being accomplished instead by tactile information. Where neuroplasticity factors into this, then, is the recruitment of one unused sensory area — in this case, the visual cortex — for processing another sense: touch. This is the activity of cross-modal plasticity: the dynamic ability for brain regions to be repurposed and adapted for other functions.
Dr. Bach-y-Rita has also utilized cross-modal plasticity in order to treat a neurological disorder caused by the antibiotic Gentamicin. In some patients, use of this medication can cause irreversible damage to the vestibular system. The inner ear houses a fluid-filled apparatus which senses the orientation of the head and projects this information to a region of the brainstem. When these connections are disturbed, a person becomes chronically uncoordinated and dizzy, incapable of knowing their orientation in space. These patients — sometimes called Wobblers — can hardly stand up or walk without falling to the ground and were considered for a long time untreatable victims of Gentamicin toxicity: a sentiment which reflected the fixed conception of the brain by orthodox neuroscience.
In order to treat these patients, Dr. Bach-y-Rita developed an accelerometer which sends its information into a plate sitting on the tongue. In this way, the patient’s brain can begin to process information relating to spatial orientation not through the vestibular apparatus, but rather through the high-density sensory neurons on the tongue. Remarkably, a series of training sessions with the device was sufficient to allow the patients to stand up and walk on their own. It appears that the spatial processing centers of the brain which once received their information from the vestibular system were now adapting, dynamically and flexibly, to receive inputs from the tongue. After training, the now-rewired brain could successfully represent the patient’s spatial orientation without the information from the damaged vestibular system.
These patients and their personal successes are a powerful example of the emerging therapeutic potential of neuroplasticity. In the next case, we’ll see an application which lies in the domain of psychodynamics: entrenched in the murky depths of human subjectivity.
Plasticity as freedom from repetition
Many have situated Freud’s discovery of unconscious processes among a succession of developments which rejected anthropocentrism. First we had Copernicus, who knocked off our seat in the middle of the solar system and situated Earth in its rightful orbit around the sun. Next was Darwin, who showed us that humanity has no unique biological origins among the animals but had evolved through the universal iron law of natural selection.
Finally, in early 20th century Vienna, a neurophysiologist-turned-clinician came to the startling conclusion that our decisions are guided by forces well outside our conscious knowledge of them. Our prize achievement — being a rational soul— had been refuted.
Jacques Lacan, a French contemporary of Freud, listed the fundamental concepts of psychodynamic theory as the unconscious, transference, drive, and repetition. It’s the last of these which most clearly conveys how psychoanalysis ‘deconstructs’ the ego and calls into question that ‘purely rational’ part of us. Repetition compulsion is a tendency for people to recreate stressful or traumatic events, frequently encountered in childhood, later in life. The mechanism for this activity, which calls to mind the ancient and mysterious concept of individual fate, is a series of automatic and unconscious interpretations of people and situations which have been preserved through time. This explains, Freud argued, why his patients sometimes acted as though he was a figure from their past, like a father or previous boss. In doing so, they were transferring their emotions from these individuals to their analyst, setting up ripe conditions for the repetition of past situations.

Doidge introduces the story of one of his patients, Mr. L, who was struggling in his late 50s after a long history with treatment-resistant depression. He would experience intermittent states of purposelessness and numbness to the world, as though everything around him was suspended in time. Most importantly for our story, he had a strained and complicated history with women. He had cheated on his ex-wife numerous times and felt blunted from emotions like love or jealousy. When he became close to a woman, he would get the sense that a better one was out there waiting for him, a feeling which contributed to his problems with commitment.
Doidge traces the source of these problems to the Mr L.’s childhood. His mother died when he was just over two years-old. Years later, he was diagnosed with a medical complication which caused him to be sent away from his father and siblings to a completely new city. Growing up in the hardened times of the Great Depression, his personal issues were never brought up or communicated to those around him. Despite this, Mr. L was not emotional or distraught when speaking about his experiences during therapy. He reported them matter-of-factly, and believed that he was too young for those influences to affect him anyway.
As psychoanalysis would predict, Mr. L’s early childhood experiences did contribute to his his psychiatric symptoms. Using his background as an analyst, Doidge ties the ideas of psychoanalysis to neuroplasticity. According to Freud, childhood is a highly ‘plastic’ period of social and sexual development. Patterns of behavior which recur and have a seemingly undefinable source can often be linked to the impressions that early childhood experiences make on our psyche. In this way, the ‘neurological imprint’ of the past event is still present even as an adult, and can cause a recurrence of certain behavioral patterns.
However, in true neuroplastic fashion, this imprint is not static and can be alleviated by obtaining insight about one’s unconscious processes. This journey of self-knowledge is facilitated by freely associating about one’s dreams and present events, which uncovers factors underlying the compulsion to repeat past circumstances.
In Mr. L’s case, a profound sense of loss could be detected through his dreamwork and associations. He often had dreams of looking for an ambiguous object which appeared to him as ‘a terrible loss’. Remarkably, the frequency of these dreams appeared to peak when his sessions were cut off by breaks or vacations. By noticing this connection between desperately searching and interruption of care, Mr. L began to realize that he wasn’t as aloof towards his mother’s death as he once thought. Eventually, he began to make a connection between his attitude towards potential love partners and these newfound feelings about his mother. The ‘potential woman out there’, the idea of which kept him from committing to any single woman, was none other than his mother, whose absence from his life was causing him a great deal of negative emotion.
Ultimately, Mr. L recognized that his behavior during adulthood was an extension of unresolved trauma from his early childhood. Although he hadn’t remembered these feelings, they were in a sense ‘living through’ him, exerting their influences unconsciously. By coming to understand himself and the psychological factors at play in his lived experience, Mr. L was able to integrate his previously-dissociated feeling and break free of the cycle which had molded his life. After years of therapy, Mr. L terminated his sessions feeling as though he “got control of his life again”.
According to Doidge, cases like these demonstrate that psychoanalysis is a kind of neuroplastic therapy. What is actually involved when a patient achieves insight into his own unconscious processes is a kind of down-regulation of certain circuits which have been imprinted by early childhood experiences. By talking through dreams and their relevant associations, a patient can come to re-transcribe these circuits by integrating them, making their symptoms less severe. In this way, Doidge presents us with the thesis that psychoanalysis and neuroplasticity bear a striking homology.
Where to next? Plasticity and the prospects of neuropsychology
As it currently stands, the relationship between neurology and psychiatry can be roughly summarized as follows. Neurologists seek to find biological sources of a symptom and will diagnose their patients accordingly; when none are found, the presenting symptoms can be considered psychogenic in nature and the patient is referred to psychiatry. In this way, the border between the specialties are drawn according to the distinction between the biological and the psychological.
But advances in neuroimaging techniques are beginning to blur this line. Now that differences in personality and behavioral traits can be mapped to morphological correlates in brain activity, the ‘biological’ may come to encompass symptoms which were previously considered purely psychological in nature. Neuroplasticity furthers this crossing over by indicating that psychiatric disorders may one day be treated with interventions which aim to rewire the brain. In short, as our understanding of the brain continues to develop, the treatments that are used may come to involve a more intimately connected union of biological and psychological intervention.
Neuropsychology, as well as its medical equivalent neuropsychiatry, are fields which seek to develop these dual treatment pathways. As our understanding of the neurobiological origin of behavior increases, we can begin to implement psychological treatments which are aimed at changing one’s neurological state as well as neurological treatments which are aimed at changing one’s psychological state. In the future, our hastily-drawn distinction between these two aspects may be seen as outdated; a relic of a time where our model of the brain was not yet clear enough.
A philosophical question lies at the center of these developments. As the strength of neuroimaging techniques increases, and neural correlates of psychological behaviors continue to mount, will we find that all of subjectivity can be reduced to a material basis? Or will there remain some unsymbolizable core at the heart of our experience: a refuge for the idea of a ‘spirit’ to reside? Developments in science and psychoanalysis removed the idea of a Cartesian ‘rational soul’. Will further development remove even the idea of a spiritual soul?
Regardless, The Brain That Changes Itself is a testament to how the power of will and resolve can literally reshape our brain, in defiance of neurological nihilism. Whether subjectivity is simply an epiphenomenon of the material or not, it’s certainly clear that our personal attitude towards healing does play a role in the upkeep of our neural connections. The patients of Dr. Bach-y-Rita and Doidge’s own psychiatric patient both confirm this idea. The knowledge that our neural constitutions are flexible may lead to a medically-grounded self-help regimen, bridging the gap between hard neuroscience and conventional wisdom. And this is a gap made closer by Doidge’s efforts, for which much praise is due.
